| Wilderness programs such as RedCliff
Ascent are relatively new forms of therapy that have not been
subjected to the same outcome and effectiveness evaluations that have
previously been performed on traditional mental health therapies.
There is a substantial body of literature on how to assess mental
health outcomes and what to expect from various therapies; however,
evaluations of wilderness programs are not a part of that literature.
In order to evaluate the effectiveness of the RedCliff Program,
independent researchers have completed the first of several
effectiveness studies which can directly answer the following
questions: What percentage of program graduates can demonstrate
significant clinical change? What long term impact does program
participation have on teens who complete the program?
 How Was It Done? How Was It Done?
A number of participants of an outdoor therapy program were
identified to provide data for the outcome study. All teens that
started the program within a several week period were included. Parent
reported measures of their teenagers mental health were gathered the
day after their son or daughter was admitted into the program.
Follow-up measures were taken 6 months later. Though most teenagers
completed the program in 5-12 weeks, it was determined that long-term
effectiveness measures would be more representative of long-term
change if the study cohort were to experience several months of
community living after completing the program. Of the original cohort
of 64 sets of parents, 91% completed both the baseline and six-month
measures.
To measure program effectiveness, an
instrument called the Youth Outcome Questionnaire (Y-OQ) was
selected. By definition, the Y-OQ is a parent reported measure of a
wide range of troublesome behaviors, situations, and moods which
commonly apply to troubled teenagers. It has demonstrated validity and
reliability and has shown high clinical sensitivity and specificity.
It is currently used in a variety of therapy settings nationally:
inpatient, residential, outpatient, day treatment, and has become the
"gold standard" for measuring youth mental health outcomes. The
instrument assesses six different sub-scales: psychosomatic,
interpersonal relations, intra-personal, social problems, behavioral
disorders, and critical items (behaviors that require immediate
medical attention ei. hallucinations and suicide). Each of the six
sub-scales are used to calculate a total Y-OQ score.
 Lets Put This in
Perspective. Lets Put This in
Perspective.
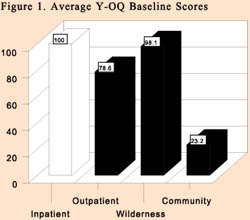
Figure 1 demonstrates the initial baseline Y-OQ scores
which were collected from several inpatient and outpatient programs,
in addition to the wilderness program and teenagers living in the
community. The average wilderness program participant had Y-OQ scores
similar to teens initiating both inpatient and outpatient treatment
programs. As shown, teens living in the community had very low scores
averaging 23.2 points. Due to the value of a standardized instrument,
we are able to compare the level of functioning of youth entering
these different treatment modalities in comparison to the community
norm.
 Did the Program Work? Did the Program Work?
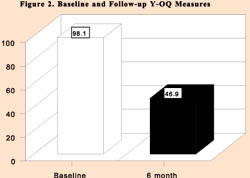
The change in Y-OQ scores that occurred to the average
wilderness program participant from baseline to six-month follow-up is
shown in Figure 2; baseline scores were cut by almost half.
Outcome findings from other mental health therapies have shown that a
13 point decrease in Y-OQ scores is considered reliable and clinically
significant. For the participants in this evaluation, 53 of 58 or
91.4% demonstrated at least a 13 point drop and were considered to
have experienced significant clinical change. Effectiveness
evaluations of other inpatient, residential, and outpatient therapies
have also shown that youth who have follow-up Y-OQ scores at or below
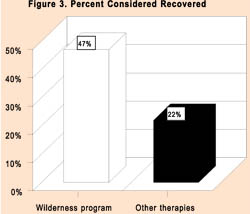
46 can be clinically labeled "recovered". In this wilderness program,
28 of the 58 students or 47% demonstrated Y-OQ follow-up scores of 46
or less. In other words, 47% of the teenagers in this cohort were
considered to be clinically recovered six months after starting the
program. How do these rates of recovery compare to recovery rates of
other traditional therapies? Y-OQ data is currently available on the
effectiveness of inpatient, residential, day treatment, and outpatient
settings. In a report that combined the overall results of these
different treatments, researchers reported that each of the therapies
were able to demonstrate some improvement in Y-OQ scores (#4). The
average recovery rate across all of these therapies was approximately
22%. Figure 3 compares the percent of wilderness program
participants who were recovered at six months with the approximate
rate of recovery for other teenagers immediately after completing
non-wilderness type therapies.
Another notable outcome was the unusually
low amount of deterioration which occurred over the six month period.
Reviews of the mental health literature have repeatedly shown that
10-12% of all patients, regardless of whether or not they are
receiving treatment, will deteriorate with time. Based upon this rate
of deterioration, 10-12% of the 58 teenagers (6-7 students) in the
study cohort could normally be expected to worsen during the six
months of the study; however, close inspection of the data revealed
that only two members of the cohort were worse after six months, and
only three failed to demonstrate significant clinical improvements.
This very low level of deterioration is atypical of most mental health
therapies.
 Conclusions Conclusions
From this outcome study, it is possible to imply that 91% of
youth who complete the program may expect to experience significant
clinical improvement in mental health status, and almost half may be
fully recovered six months after initiating the program. Because the
study design was not a randomized
 clinical trial, it is
impossible to prove that the program is solely responsible for these
improvements in mental health. Despite this limitation, it is obvious
that the program is responsible for most, if not all of the dramatic
improvements demonstrated. clinical trial, it is
impossible to prove that the program is solely responsible for these
improvements in mental health. Despite this limitation, it is obvious
that the program is responsible for most, if not all of the dramatic
improvements demonstrated.
REFERENCES
1. American Professional Credentialing Services LLC, Youth
Outcomes Questionnaire,(1996).
2. Wells, M.G., et al. (1996). Conceptualization and measurement of
patient change during psychotherapy: Development of the Youth and
Adult Outcome Questionnaires, Psychotherapy: Theory, Research, and
Practice, 33(2),275-283.
3. Tingey, R., et al. (1996). Clinically significant change: Practical
indicators for evaluating psychotherapy outcome. Psychotherapy
Research, 6(2),144-153.
4. Berrett, K.M., (August, 1998) Youth Outcome Questionnaire (Y-OQ):
Item sensitivity to change. Paper presented at the Annual Meeting of
the American Psychological Association. San Francisco, CA.
This research was conducted by Dr. Steven
G. Aldana, a research design specialist and professor in the College
of Health and Human Performance of Brigham Young University. Inquiries
regarding this research may be directed to him by email or phone:
steve_aldana@byu.edu (801)378-2145 |
